
Changes in the microstructure and bone mineral density of vertebral trabecular bone in the early stages of spinal Mycobacterium tuberculosis infection
-
摘要:
目的 观察比较脊柱结核分枝杆菌感染早期椎体骨密度的变化。 方法 连续收集2023年1月1日—12月31日就诊于中南大学湘雅医院脊柱外科的脊柱结核手术患者(脊柱结核组), 依据性别匹配椎管狭窄就诊的非脊柱结核手术患者为对照组。对入组患者进行双能X线扫描, 比较两组患者椎体骨密度的差异。构建脊柱结核分枝杆菌感染动物模型(简称动物模型), 比较动物模型脊柱结核组与对照组的骨小梁微结构差异, 选择骨组织/体积骨量(BV/TV)、骨小梁厚度(Tb.Th)、骨小梁数量(Tb.N)和骨小梁分离度(Tb.Sp)作为评价指标, 进一步分析病椎与邻椎的骨质差异。 结果 脊柱结核组和对照组分别纳入69例患者, 脊柱结核组患者骨密度[0.793(0.712, 0.869) g/cm2]低于对照组[0.907(0.800, 1.020) g/cm2], 差异有统计学意义(P<0.05)。动物模型脊柱结核组小鼠的骨小梁微结构BV/TV[(18.4±5.4)%]、Tb.Th [(0.124±0.010) mm]较对照组BV/TV[(22.6±3.2)%]、Tb.Th [(0.160±0.017) mm]发生明显改变(均P<0.05)。动物模型脊柱结核组中, 小鼠病椎骨小梁微结构BV/TV[(25.5±6.7)%]、Tb.N[(1.871±0.443)/mm]低于邻椎的BV/TV[(26.6±6.8)%]、Tb.N [(1.969±0.454)/mm], 差异均有统计学意义(均P<0.05)。 结论 结核分枝杆菌感染椎体早期可引起骨小梁微结构发生改变, 进而导致骨密度降低。 Abstract:Objective To observe and compare the changes of vertebral bone mineral density (BMD) in the early stages of spinal Mycobacterium tuberculosis infection. Methods Patients who underwent spinal surgery at Xiangya Hospital, Central South University from January 1 to December 31, 2023 were continuously enrolled (spinal tuberculosis group), based on gender matching, non-spinal tuberculosis surgical patients treated for spinal stenosis were selected as the control group. Dual-energy X-ray scans were performed on the enrolled patients, difference in vertebral BMD between two groups of patients was compared. An animal model of spinal Mycobacterium tuberculosis infection (referred to as the animal model) was constructed, differences in microstructure of trabecular bone between spinal tuberculosis group and control group was compared, and the bone volume/tissue volume (BV/TV), the thickness of trabecular bone (Tb.Th), the number of trabecular bone (Tb.N), and sparse density of trabecular (Tb.Sp) were used as evaluation indexes to further analyze the bone quality differences between the diseased vertebrae and the neighboring vertebrae. Results 69 patients were included in the spinal tuberculosis group and the control group, respectively. The BMD of patients in the spinal tuberculosis group (0.793 [0.712, 0.869] g/cm2) was lower than that of the control group (0.907 [0.800, 1.020] g/cm2), difference was statistically significant (P < 0.05). Microstructure of trabecular bone BV/TV ([18.4±5.4]%), Tb.Th ([0.124±0.010] mm) in the spinal tuberculosis group of animal model were significantly altered compared with BV/TV ([22.6±3.2]%), Tb.Th ([0.160±0.017] mm) in the control group (both P < 0.05). In the spinal tuberculosis group, microstructure of diseased vetebral trabecular bone BV/TV ([25.5±6.7]%) and Tb.N ([1.871±0.443]/mm) were significantly lower than BV/TV ([26.6±6.8]%) and Tb.N ([1.969±0.454]/mm) in the neighboring vertebrae, both with statistically difference (both P < 0.05). Conclusion In the early stages of spinal Mycobacterium tuberculosis infection, microstructure of vertebral trabecular bone can be altered, leading to a decrease in BMD. -
据世界卫生组织(WHO)统计,全球结核病发病率在2021—2022年连续两年上升,而我国结核病例占全球结核病病例的比率高达7.1%[1]。结核分枝杆菌感染具有潜伏期较长、难以诊断等特点[2]。结核分枝杆菌感染椎体导致脊柱结核,随病程进展,感染椎体逐渐出现骨质丢失、骨质破坏、病理性成骨,乃至死骨的形成[3]。脊柱结核的症状多以疼痛、活动障碍为主,病变进一步发展可导致畸形或截瘫[4]。但脊柱结核的早期诊断存在一定困难,经常存在漏诊与误诊[5]。脊柱结核的CT、磁共振(MRI)与多层螺旋CT(MSCT)等影像学资料表现多样[6-7],确诊仍依赖于手术活检及结核分枝杆菌培养。研究[8-9]证实,结核分枝杆菌可通过多种途径干扰骨代谢,导致局部乃至全身的成骨与破骨失衡,最终表现为骨质破坏。因此,研究脊柱结核分枝杆菌感染早期椎骨骨质微结构改变,对明确早期诊断有重大意义。目前,micro CT已经广泛应用于小梁骨和皮质骨形态的研究[10-11]中,其中,骨组织/体积骨量(bone volume/tissue volume, BV/TV)、骨小梁厚度(thickness of trabecular bone, Tb.Th)、骨小梁数量(number of trabecular bone, Tb. N)和骨小梁分离度(sparse density of trabecular, Tb. Sp)是评价骨小梁微结构的主要指标[12]。本研究连续收集脊柱结核患者资料,分析比较其与对照组的骨密度差异,并采用结核分枝杆菌感染小鼠椎体,构建脊柱结核动物模型,通过评价骨小梁微结构,进一步比较脊柱结核分枝杆菌感染组与对照组病椎和邻椎骨密度差异。
1. 对象与方法
1.1 研究对象
1.1.1 脊柱结核患者与对照组患者
连续收集2023年1月1日—12月31日就诊于中南大学湘雅医院脊柱外科的脊柱结核手术患者资料(脊柱结核组),依据性别匹配椎管狭窄就诊的非脊柱结核手术患者为对照组。脊柱结核组纳入标准: ①患者脊柱病灶组织标本经结核分枝杆菌培养、结核分枝杆菌耐药检测(Xpert)、宏基因组二代测序技术(mNGS)检测,最终确定为结核分枝杆菌感染;②骨密度资料完善;③年龄在15~75岁。对照组纳入标准:①因椎管狭窄就诊的非脊柱结核手术患者;②性别与脊柱结核组相匹配;③骨密度资料完善;④年龄在15~75岁。排除标准: ①脊柱多重感染者;②有严重的全身性疾病者,如风湿、自身免疫病、肝肾功能不全等;③肿瘤患者。
1.1.2 试验动物
SPF级8周龄、C57BL/6雌性小鼠共10只,均购自湖南博睿鑫生物科技有限公司。随机分为试验组(n=5)与对照组(n=5),试验组与对照组小鼠造模前2周,使用弗氏完全佐剂0.1 mL腹腔注射致敏,1次/周,致敏2周后开始造模。
1.2 结核分枝杆菌的准备
结核分枝杆菌减毒株H37Ra(购自上海晶诺生物科技有限公司),采用罗氏培养基培养1个月后,使用0.9% 的灭菌生理盐水重悬菌落,采用比浊法配置成浓度为108 CFU/mL的结核分枝杆菌悬液,再与Matrigel Matrix基质胶按照3 ∶1比例配置成注射用菌悬液,备用。
1.3 构建动物模型
造模方法参照高琪乐等[13]在2018年建立的注射的方法,即小鼠使用弗氏完全佐剂致敏2周后,使用10%水合氯醛3 mL/kg进行腹腔注射麻醉。动物模型结核组注射0.1 mL混合胶的菌悬液,将注射位置由小鼠椎体改为小鼠尾骨,完成注射后针头停留30~60 s,待胶凝固后,拔出针头。以上试验均在上海晶诺生物科技有限公司生物安全实验室进行。动物模型对照组注射0.1 mL Matrigel Matrix基质胶,其余操作同动物模型结核组。
1.4 Micro CT检测
造模3周后,将动物模型小鼠尾用micro CT扫描仪(SCANCO Micro CT viva CT 40)扫描,采用CT vox进行三维重建,CT an比较病椎和邻椎的骨微结构,选择BV/TV、Tb.Th、Tb.N、Tb.Sp作为评价指标[12]。
1.5 骨密度检测
脊柱结核组与对照组均采用双能X线骨密度仪检查,测量腰椎L1~L4的骨密度,并比较L1~L4的平均骨密度。病椎位置由MRI确定。邻椎选取病椎相邻上位或下位腰椎椎体。手术组医生术中取脊柱结核病灶标本送病理检查和微生物学检查(抗酸染色、结核分枝杆菌培养、Xpert、mNGS)进一步确定病椎和对照邻椎。
1.6 统计学分析
数据分析与作图应用GraphPad Prism 9.0统计软件。计数资料采用卡方检验,计量资料经Shapiro-Wilk test检验呈正态分布时,以x±s表示;不符合正态分布时,以M(Q1, Q3)表示,检验方法采用非参数检验。配对资料采用配对样本t检验。以P≤0.05为差异有统计学意义。
2. 结果
2.1 脊柱结核组与对照组患者的骨密度
脊柱结核组、对照组分别纳入患者69例。两组患者年龄比较,差异无统计学意义(P>0.05),但脊柱结核组患者L1~L4的平均骨密度低于对照组(P<0.001)。见表 1。
表 1 脊柱结核组与对照组患者的年龄及骨密度检查结果Table 1 Age and BMD examination results of patients in spinal tuberculosis group and control group项目 脊柱结核组(n=69) 对照组(n=69) 正秩总和 负秩总和 Z P 年龄[M(Q1, Q3), 岁] 60.00(53.50, 69.00) 57.00(51.00, 63.50) 1 032 1 383 -1.05 0.297 L1~L4平均骨密度[M(Q1, Q3),g/cm2] 0.793(0.712, 0.869) 0.907(0.800, 1.020) 1 989 426 -4.67 <0.001 2.2 动物模型脊柱micro CT的骨质检查结果
对动物模型结核组、对照组小鼠尾椎micro CT扫描结果应用软件CT vox进行三维重建,结果显示,动物模型结核组小鼠尾椎均可见较为明显的骨质破坏病灶,动物模型对照组未见明显骨质破坏灶。见图 1。
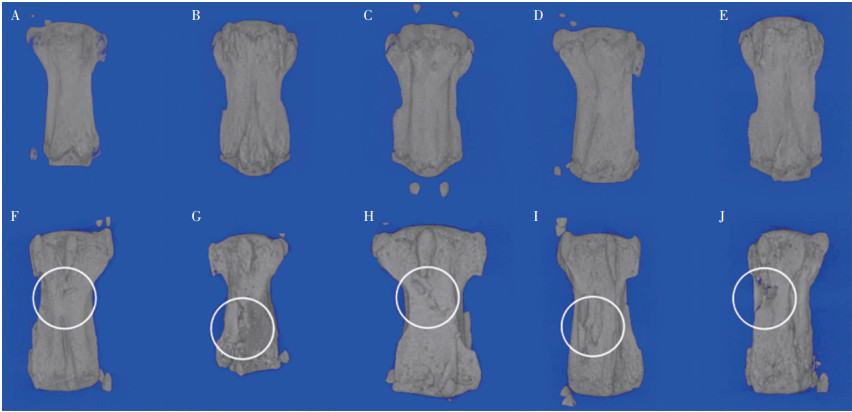 图 1 动物模型脊柱micro CT扫描三维重建图像注:A~E为对照组,F~J为结核组。Fig. 1 Spinal micro CT three-dimensional reconstruction images of the animal model
图 1 动物模型脊柱micro CT扫描三维重建图像注:A~E为对照组,F~J为结核组。Fig. 1 Spinal micro CT three-dimensional reconstruction images of the animal model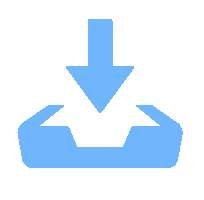 下载:
全尺寸图片
下载:
全尺寸图片
2.3 动物模型结核组与对照组micro CT骨小梁微结构检测结果
每只小鼠选择注射椎体及其上下相邻椎体共3节进行分析,应用软件CT an对所选节段的BV/TV、Tb.Th、Tb.N和Tb.Sp平均值进行分析,结果显示,动物模型结核组小鼠的BV/TV、Tb.Th均低于动物模型对照组小鼠(均P<0.05),而动物模型结核组与对照组的Tb.N、Tb.Sp比较,差异均无统计学意义(均P>0.05),见表 2。
表 2 动物模型结核组和对照组的骨小梁微结构检测结果(x±s)Table 2 Microstructural examination results of trabeculae bone in tuberculosis and control groups of animal model (x±s)检测指标 结核组(n=5) 对照组(n=5) t P BV/TV(%) 18.4±5.4 22.6±3.2 2.606 0.015 Tb.Th (mm) 0.124±0.010 0.160±0.017 7.050 <0.001 Tb.N (1/mm) 1.473±0.364 1.423±0.200 0.469 0.643 Tb.Sp (mm) 0.642±0.166 0.636±0.051 0.134 0.894 2.4 动物模型结核组病椎与邻椎micro CT三维重建及其骨小梁微结构分析结果
应用软件CTan对动物模型结核组小鼠病椎与邻椎的BV/TV、Tb.Th、Tb.N和Tb.Sp进行分析,发现病椎的BV/TV[(25.5±6.7)%]、Tb.N[(1.871±0.443)/mm]低于邻椎的BV/TV[(26.6±6.8)%]、Tb.N [(1.969±0.454) /mm;均P<0.05],而病椎和邻椎的Tb.Th、Tb.Sp比较,差异均无统计学意义(均P>0.05)。见表 3。动物模型结核组病椎与邻椎的micro CT三维重建图像见图 2。
表 3 动物模型结核组小鼠病椎和邻椎的骨小梁微结构检测结果(x±s)Table 3 Microstructural examination results of trabeculae bone of diseased vertebrae and neighboring vertebrae in tuberculosis group of animal model (x±s)检测指标 病椎(n=5) 邻椎(n=5) 差值95%CI t P BV/TV(%) 25.5±6.7 26.6±6.8 (0.005, 0.017) 4.757 0.009 Tb.Th (mm) 0.136±0.008 0.134±0.008 (-0.006, 0.003) 0.829 0.454 Tb.N (1/mm) 1.871±0.443 1.969±0.454 (0.020, 0.177) 3.483 0.025 Tb.Sp (mm) 0.539±0.115 0.547±0.136 (-0.022, 0.038) 0.709 0.517  图 2 动物模型结核组病椎与邻椎的micro CT三维重建图像注:A、B、C、D、E分别为结核组5只小鼠的病椎与邻椎,放大图为病椎。Fig. 2 Micro CT three-dimensional reconstruction images of the diseased vertebrae and neighboring vertebrae in tuberculosis group of animal model下载:
全尺寸图片
图 2 动物模型结核组病椎与邻椎的micro CT三维重建图像注:A、B、C、D、E分别为结核组5只小鼠的病椎与邻椎,放大图为病椎。Fig. 2 Micro CT three-dimensional reconstruction images of the diseased vertebrae and neighboring vertebrae in tuberculosis group of animal model下载:
全尺寸图片
2.5 腰椎脊柱结核患者感染早期的骨密度信息
选择就诊于中南大学湘雅医院的腰椎脊柱结核病程≤3个月的患者共9例,对其骨密度资料进行分析,发现病椎骨密度(0.815±0.111)g/cm2低于邻椎(0.874±0.123)g/cm2,两者比较差异有统计学意义(t=6.109, P<0.001)。
3. 讨论
对2023年1月1日—12月31日就诊于中南大学湘雅医院的脊柱结核患者进行研究,发现脊柱结核患者骨密度低于对照组。为进一步验证骨密度的改变是否由结核分枝杆菌感染导致,本研究通过结核分枝杆菌H37Ra感染小鼠3周,构建早期脊柱结核分枝杆菌感染模型,发现动物模型结核组的骨小梁微结构较对照组有明显改变,BV/TV与Tb.Th均明显降低。此外,进一步分析脊柱结核病椎与邻椎之间的骨小梁微结构差异性,动物模型脊柱结核组小鼠检查结果显示,病椎的骨小梁体积分数及骨小梁的数量均低于其相邻椎体,差异具有统计学意义,即病椎的骨小梁微结构差于邻椎,在对短病程脊柱结核患者病椎与邻椎的研究中也发现,病椎骨密度较邻椎骨密度明显降低。
已经有研究[14-15]表明,脊柱结核患者的骨密度会出现明显的降低,骨质疏松及骨不良事件的发生率明显高于正常人群[16],此点在本研究中进一步得到验证。动物试验中,高琪乐等[13]在脊柱结核造模中发现,脊柱结核椎体Tb.N与Tb.Th显著降低,病灶周围椎体Tb.N与Tb.Th增加。本组动物试验研究借鉴了其在2018年采用的方法[13],但将注射部位由小鼠脊柱椎体改为小鼠尾椎骨,进一步提高了造模的成模率,并且在对动物模型结核组与对照组骨小梁微结构差异进行分析的基础上,进一步分析病椎与其相邻椎体之间的差异,更加明确地证实了结核分枝杆菌感染导致椎体骨小梁微结构发生改变。由于动物试验造模时间为3周,考虑脊柱结核分枝杆菌感染处于早期,为了匹配病程,临床选择短病程(≤3个月)患者进行骨密度差异性分析,发现病椎骨密度较邻椎骨密度明显降低,与动物试验结果相符,推测在脊柱结核分枝杆菌感染早期,病理改变以骨质破坏为主,导致椎体骨密度较邻椎降低[14]。而随着时间的推移与疾病的进展,逐渐有病理性成骨及死骨的形成[17],病椎骨密度也可能出现进一步的改变。也有研究[18]发现,脊柱结核的病理性成骨比化脓性脊柱炎更加显著,表明结核分枝杆菌导致骨感染后不仅导致骨质破坏,且有病理性成骨的形成。
本研究对脊柱结核组与对照组患者的骨密度研究为前瞻性研究,入组病例按随机原则选取,避免了以往回顾性研究存在的偏倚。用于致病的结核分枝杆菌是减毒株H37Ra,其毒力及对巨噬细胞的激活作用虽然弱于H37Rv[19-20],但仍能导致骨代谢的改变,并广泛应用于结核分枝杆菌与骨代谢相关性的研究中[8, 21]。本研究不仅比较脊柱结核患者与对照组,更进一步聚焦于结核组病椎和邻椎之间的骨密度差异,避免了个体差异带来的影响,有效避免了偏倚,并发现结核分枝杆菌感染导致骨密度的降低早期集中于病椎。由于造模时间的限制,本研究未能观察到长病程脊柱结核感染后椎体骨微结构的改变情况;同时由于本院双能骨密度检测仅限于腰椎节段,因此部分颈椎、胸椎结核的临床患者并未被纳入研究。此外,临床患者评价指标采用双能X线骨密度仪测量骨密度,其精度与准确度不如定量CT(QCT)[22],在后续的研究中,也将使用QCT更为全面地评价患者骨密度。
综上所述,结核分枝杆菌感染椎体可导致椎体骨小梁微结构的改变。脊柱结核患者病椎改变早期以骨密度降低为主。但病椎与邻椎骨密度随感染时间增加的变化趋势尚不清楚。后续试验中将纳入更多样本,采用更多的评价指标以评估长病程感染后椎体骨小梁微结构及椎体骨密度的变化。
-
图 1 动物模型脊柱micro CT扫描三维重建图像
注:A~E为对照组,F~J为结核组。
Fig. 1 Spinal micro CT three-dimensional reconstruction images of the animal model
下载:
全尺寸图片
图 2 动物模型结核组病椎与邻椎的micro CT三维重建图像
注:A、B、C、D、E分别为结核组5只小鼠的病椎与邻椎,放大图为病椎。
Fig. 2 Micro CT three-dimensional reconstruction images of the diseased vertebrae and neighboring vertebrae in tuberculosis group of animal model
下载:
全尺寸图片
表 1 脊柱结核组与对照组患者的年龄及骨密度检查结果
Table 1 Age and BMD examination results of patients in spinal tuberculosis group and control group
项目 脊柱结核组(n=69) 对照组(n=69) 正秩总和 负秩总和 Z P 年龄[M(Q1, Q3), 岁] 60.00(53.50, 69.00) 57.00(51.00, 63.50) 1 032 1 383 -1.05 0.297 L1~L4平均骨密度[M(Q1, Q3),g/cm2] 0.793(0.712, 0.869) 0.907(0.800, 1.020) 1 989 426 -4.67 <0.001 表 2 动物模型结核组和对照组的骨小梁微结构检测结果(x±s)
Table 2 Microstructural examination results of trabeculae bone in tuberculosis and control groups of animal model (x±s)
检测指标 结核组(n=5) 对照组(n=5) t P BV/TV(%) 18.4±5.4 22.6±3.2 2.606 0.015 Tb.Th (mm) 0.124±0.010 0.160±0.017 7.050 <0.001 Tb.N (1/mm) 1.473±0.364 1.423±0.200 0.469 0.643 Tb.Sp (mm) 0.642±0.166 0.636±0.051 0.134 0.894 表 3 动物模型结核组小鼠病椎和邻椎的骨小梁微结构检测结果(x±s)
Table 3 Microstructural examination results of trabeculae bone of diseased vertebrae and neighboring vertebrae in tuberculosis group of animal model (x±s)
检测指标 病椎(n=5) 邻椎(n=5) 差值95%CI t P BV/TV(%) 25.5±6.7 26.6±6.8 (0.005, 0.017) 4.757 0.009 Tb.Th (mm) 0.136±0.008 0.134±0.008 (-0.006, 0.003) 0.829 0.454 Tb.N (1/mm) 1.871±0.443 1.969±0.454 (0.020, 0.177) 3.483 0.025 Tb.Sp (mm) 0.539±0.115 0.547±0.136 (-0.022, 0.038) 0.709 0.517 -
[1] World Health Organization. Global tuberculosis report 2023[EB/OL]. (2023-11-07)[2024-02-10]. https://www.who.int/publications/i/item/9789240083851. [2] Boom WH, Schaible UE, Achkar JM. The knowns and unknowns of latent Mycobacterium tuberculosis infection[J]. J Clin Invest, 2021, 131(3): 136222. doi: 10.1172/JCI136222 [3] 石广灿. 不同影像学方法在诊断脊柱结核中的应用[J]. 中国CT和MRI杂志, 2018, 16(6): 131-133. doi: 10.3969/j.issn.1672-5131.2018.06.040 Shi GC. Application of different imaging methods in diagnosis of spinal tuberculosis[J]. Chinese Journal of CT and MRI, 2018, 16(6): 131-133. doi: 10.3969/j.issn.1672-5131.2018.06.040 [4] 中华医学会结核病分会骨科专业委员会. 中国脊柱结核外科治疗指南(2022年版)[J]. 中国矫形外科杂志, 2022, 30(17): 1537-1548. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS202217018.htm Orthopaedic Professional Committee of Chinese Society for Tuberculosis, Chinese Medical Association. Chinese guidelines for surgical management of spinal tuberculosis (2022 edition)[J]. Orthopedic Journal of China, 2022, 30(17): 1537-1548. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS202217018.htm [5] Mann TN, Davis JH, Walzl G, et al. Candidate biomarkers to distinguish spinal tuberculosis from mechanical back pain in a tuberculosis endemic setting[J]. Front Immunol, 2021, 12: 768040. doi: 10.3389/fimmu.2021.768040 [6] Liu XY, Zheng MM, Sun JM, et al. A diagnostic model for differentiating tuberculous spondylitis from pyogenic spondylitis on computed tomography images[J]. Eur Radiol, 2021, 31(10): 7626-7636. doi: 10.1007/s00330-021-07812-1 [7] 王姿丽, 梁昆, 杨长成. 脊柱结核骨质破坏、脓腔MSCT、MRI特点与临床病程的关系研究[J]. 重庆医学, 2023, 52(24): 3779-3784. https://www.cnki.com.cn/Article/CJFDTOTAL-CQYX202324019.htm Wang ZL, Liang K, Yang CC. Study on the relationship between MSCT and MRI features of bone destruction, pus cavity and clinical course of spinal tuberculosis[J]. Chongqing Medicine, 2023, 52(24): 3779-3784. https://www.cnki.com.cn/Article/CJFDTOTAL-CQYX202324019.htm [8] Ma WX, Jin WD, He XJ, et al. Mycobacterium tuberculosis induced osteoblast dysregulation involved in bone destruction in spinal tuberculosis[J]. Front Cell Infect Microbiol, 2022, 12: 780272. doi: 10.3389/fcimb.2022.780272 [9] Deng JZ, Yang YS, He JY, et al. Vitamin D receptor activated by vitamin D administration alleviates Mycobacterium tuberculosis-induced bone destruction by inhibiting NFκB-mediated aberrant osteoclastogenesis[J]. FASEB J, 2021, 35(6): e21543. [10] Hu SY, Li HM, Jiang HH, et al. Macrophage activation in synovitis and osteoarthritis of temporomandibular joint and its relationship with the progression of synovitis and bone?remodeling[J]. Am J Pathol, 2024, 194(2): 296-306. doi: 10.1016/j.ajpath.2023.11.010 [11] Ding ZB, Chen Y, Zheng YR, et al. Inhibition of PPP1R15A alleviates osteoporosis via suppressing RANKL-induced osteo-clastogenesis[J]. Acta Pharmacol Sin, 2024, 45(4): 790-802. doi: 10.1038/s41401-023-01209-0 [12] Bouxsein ML, Boyd SK, Christiansen BA, et al. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography[J]. J Bone Miner Res, 2010, 25(7): 1468-1486. doi: 10.1002/jbmr.141 [13] 高琪乐, 张宏其, 郭超峰, 等. 小鼠脊柱结核模型的构建及椎体骨密度改变的初步研究[J]. 中国矫形外科杂志, 2018, 26(2): 155-158. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS201802016.htm Gao QL, Zhang HQ, Guo CF, et al. Bone density changes of trabecular bone in spinal tuberculosis murine model[J]. Orthopedic Journal of China, 2018, 26(2): 155-158. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS201802016.htm [14] 安晋宇, 李大伟, 崔旭, 等. 脊柱结核与骨量减低相关研究[J]. 中国骨与关节外科, 2013, 6(2): 145-147, 152. doi: 10.3969/j.issn.1674-1439.2013.04-011 An JY, Li DW, Cui X, et al. Correlation between spine tuberculosis and bone mass[J]. Chinese Journal Bone and Joint Surgery, 2013, 6(2): 145-147, 152. doi: 10.3969/j.issn.1674-1439.2013.04-011 [15] 郭超峰, 胡小江, 李韬, 等. 脊柱结核患者骨密度与骨髓间充质干细胞迁徙研究[J]. 中国感染控制杂志, 2022, 21(8): 762-767. http://www.zggrkz.com/zggrkzzz/article/abstract/2022-8-762?st=search Guo CF, Hu XJ, Li T, et al. Bone mineral density and migration of bone marrow mesenchymal stem cells in patients with spinal tuberculosis[J]. Chinese Journal of Infection Control, 2022, 21(8): 762-767. http://www.zggrkz.com/zggrkzzz/article/abstract/2022-8-762?st=search [16] Chen YY, Feng JY, Ting WY, et al. Increased risk of incident osteoporosis and osteoporotic fracture in tuberculosis patients: a population-based study in a tuberculosis-endemic area[J]. Osteoporos Int, 2017, 28(5): 1711-1721. doi: 10.1007/s00198-017-3939-x [17] 杨海青, 段洪. 脊柱结核病理及影像学形态多样性特征[J]. 实用骨科杂志, 2015, 21(5): 473-476. https://www.cnki.com.cn/Article/CJFDTOTAL-SGKZ201505037.htm Yang HQ, Duan H. Multiform character of imaging and patho- logical in spinal tuberculosis[J]. Journal of Practical Orthopaedics, 2015, 21(5): 473-476. https://www.cnki.com.cn/Article/CJFDTOTAL-SGKZ201505037.htm [18] 李石磊, 张宏其, 李韬, 等. 脊柱结核与化脓性脊柱炎全身与局部骨结构比较[J]. 中国矫形外科杂志, 2022, 30(10): 920-924. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS202210012.htm Li SL, Zhang HQ, Li T, et al. Comparison of systemic and local bone structures in spinal tuberculosis and suppurative spondylitis[J]. Orthopedic Journal of China, 2022, 30(10): 920-924. https://www.cnki.com.cn/Article/CJFDTOTAL-ZJXS202210012.htm [19] Li AH, Waddell SJ, Hinds J, et al. Contrasting transcriptio-nal responses of a virulent and an attenuated strain of Mycobacterium tuberculosis infecting macrophages[J]. PLoS One, 2010, 5(6): e11066. doi: 10.1371/journal.pone.0011066 [20] Roach TI, Barton CH, Chatterjee D, et al. Macrophage activation: lipoarabinomannan from avirulent and virulent strains of Mycobacterium tuberculosis differentially induces the early genes c-fos, KC, JE, and tumor necrosis factor-alpha[J]. J Immunol, 1993, 150(5): 1886-1896. doi: 10.4049/jimmunol.150.5.1886 [21] Li XJ, He LG, Hu YP, et al. Sinomenine suppresses osteoclast formation and Mycobacterium tuberculosis H37Ra-induced bone loss by modulating RANKL signaling pathways[J]. PLoS One, 2013, 8(9): e74274. [22] Engelke K, Libanati C, Liu Y, et al. Quantitative computed tomography (QCT) of the forearm using general purpose spiral whole-body CT scanners: accuracy, precision and comparison with dual-energy X-ray absorptiometry (DXA)[J]. Bone, 2009, 45(1): 110-118. doi: 10.1016/j.bone.2009.03.669
